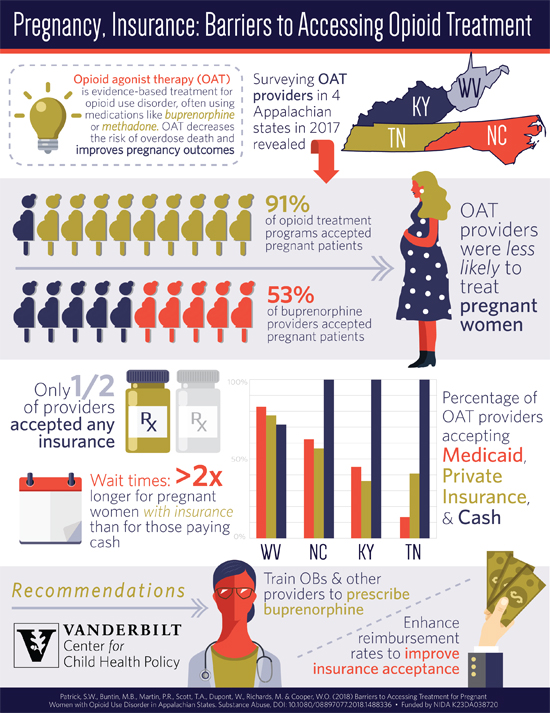
NewsStudy Reveals Opioid Patients Face Multiple Barriers to TreatmentIn areas of the country disproportionately affected by the opioid crisis, treatment programs are less likely to accept patients paying through insurance of any type or accept pregnant women, a new Vanderbilt study found. While the opioid crisis has escalated across the United States, there has been growing concern that treatment capacity has not kept pace. In 2016, more than 42,000 Americans died of an opioid-related overdose, more than any year on record. Opioid agonist therapies, like buprenorphine and methadone, have been shown to reduce risk of overdose death, and for pregnant women with opioid use disorder this benefit extends to the baby—making it more likely the infant will be born at term and with higher birthweights. Vanderbilt researchers focused on four Appalachian states—Tennessee, Kentucky, North Carolina, and West Virginia—that have among the highest rates of opioid use in the country and are more affected by opioid overdose deaths. In their study published in the journal Substance Abuse, researchers found that only about 50% of opioid treatment providers took any insurance, and there was also a huge variance among the states in programs that accepted Medicaid. While 83% of treatment programs in West Virginia accepted Medicaid insurance, only about 13% of programs in Tennessee accepted Medicaid. Additionally, the study found that while 91% of programs were accepting new patients, only 53% of outpatient buprenorphine would treat pregnant women. "This work sheds further light on a critical public health problem facing pregnant women and their children and the importance of connecting pregnant women to the right resources," says senior author William Cooper, MD, MPH, vice chair of the department of pediatrics and Cornelius Vanderbilt Professor of Pediatrics and Health Policy. Researchers conducted a survey of opioid agonist therapy providers, opioid treatment programs that provide methadone and outpatient buprenorphine providers between April and May 2017, in the four predominately Appalachian states. The programs and providers were identified from a public listing provided by the Substance Abuse and Mental Health Administration. "We know that opioid agonist therapies work but only a fraction of people that have opioid use disorder are actually getting them. With this study, we wanted to know if there were structural issues in terms of providers, or insurance type, or being pregnant itself, that may be a reason for that barrier," says Stephen W. Patrick, MD, MPH, MS, director of the Vanderbilt Center for Child Health Policy, and an assistant professor of pediatrics and health policy in the division of neonatology at Monroe Carell Jr. Children's Hospital at Vanderbilt. Surveyors asked the programs if they were accepting new patients or if they were accepting pregnant patients for treatment. Other questions centered on insurance requirements, including if programs accepted Medicaid, private insurance, or self-pay. The survey found that cash payments for treatment ranged from $20 to $175 for treatment intakes, $35 to $245 per week for outpatient buprenorphine treatment, and $49 to $160 per week for methadone treatment. Another finding of the study was that when pregnant women are accepted to opioid use disorder treatment programs they had shorter wait times than others with the disorder. "We need to know why—why is it that so many providers only take cash and why so few in some states take Medicaid. Then we need to craft policy solutions that increase the likelihood that people with opioid use disorder are able to get the evidence-based treatment that they need," Patrick says. "At the end of the day, the people that have opioid use disorder, particularly pregnant women, need the treatment that we know is evidence based. We know many aren't getting it and we are still seeing record highs of overdose deaths." Source: Vanderbilt University Medical Center
Photo Credit: Department of Health Policy, Vanderbilt University School of Medicine |

Great Valley Publishing Company
1721 Valley Forge Road #486
Valley Forge, PA 19481
1721 Valley Forge Road #486
Valley Forge, PA 19481