|
Results from a nurturing parenting program reveal where work needs to be done. In the United States, four children die each day from maltreatment (Evans et al., 2014) and 6 million referrals are made annually to child protection agencies concerning some form of alleged abuse of children (Peterson et al., 2018). The latter statistic continues to grow—as of 2017, an estimated 37.4% of all children experience a child protective services investigation by age 18 (Kim et al., 2017). Child maltreatment has been shown to be connected with higher levels of relationship issues throughout the child’s life (Bailey et al., 2007); posttraumatic stress (Stovall-McClough & Cloitre, 2006); a distorted view of self, others, and the world (Lo et al., 2019); and disrupted interactive behavior with their own children (Madigan et al., 2007), creating a cyclical pattern when left unaddressed. Child welfare agencies can become involved with families that demonstrate high risk of maltreatment due to substantiated allegations of abuse, neglect, or substance use. The child may then be removed from the home, and/or services may be implemented with the goal of reducing risk of further maltreatment and to facilitate stability within the family unit. The goal of preventive services is to help families build and reinforce protective factors to reduce risk of child maltreatment, child removal, and out-of-home foster placement, thereby eliminating the need for systematic and repetitive welfare involvement as well as mitigating the negative residual effects accompanied by abuse. Home visitation programs that intervene in high-risk families provide services to assist in reducing risk of child maltreatment (Olds et al., 2004). This article examines the impacts of one agency’s service delivery of the Nurturing Parenting home visiting program on protective factors in families at risk of child maltreatment. Methods The treatment “dosage” in terms of the frequency, duration of each session, and length of the intervention is determined based on family risk level, which is assessed by the Adult-Adolescent Parenting Inventory (AAPI). Families that are identified as having higher risk levels are prescribed higher “dosages” of the intervention. Each competency is targeted toward reinforcing one of the following protective factors: expectations of children, parental empathy toward children’s needs, use of corporal punishment, parent-child family roles, and children’s power and independence (Bavolek & Keene, 1999). Lessons are designed to be delivered in a sequential manner. The framework for each lesson includes the following: the title of the lesson and lesson number, the correlating construct the lesson targets, a description of the lesson, the expected competencies developed from the lesson, prerequisites (lessons the parent needs to have completed before beginning the specified lesson), materials needed for the lesson, teaching goals, lesson procedures, the home practice assignment (homework for the families to complete before the next session), family nurturing time (attachment informed activity), notes and suggestions, and home visitor notes (Bavolek, 2006). The home visit ends with a review of the session and an evaluation of the demonstrated competencies. These evaluations are made collaboratively by both the staff member and the parent who work together to assess the parent’s capability in the competency targeted in each lesson before moving on to the next lesson. Sample Parent ages ranged from 16 to 79 with an average age of 30. Regarding gender, 19% of participants were male and 81% were female. Family size in this sample varied, with between one and 10 children residing in the home. The most common number of children in the home where services were provided was two (36%). Marital status varied as well, with the most commonly reported status being single parents (never married; 54%). The majority of the participants in this sample identified as either white (47%) or Black (36%). Income ranges varied with the most common level being under $15,000 annually (38%). Within this sample, the most common response to education level was some college (28%), followed closely by high school graduate with no college (26%). The two most commonly reported employment statuses were working full time (30%) and unemployed (21%). It is noteworthy that the choice “stay-at-home parent” is differentiated from “unemployed” within employment identification (see Table 1).
Procedure The initial data set included all pre- and posttest scores on the AAPI collected from the most recently completed fiscal year (July 2018 to June 2019), which yielded a total of 148 participants. The AAPI, a validated self-report tool that assesses five protective factor domains in families, is completed by the client at baseline prior to any intervention delivery and then again post intervention. Each factor’s total score is determined by multiple subscale scores answered by the parents assessed. Pretest scores from 36 participants were collected with no corresponding posttest. This was either due to dropout or completing the posttest after the cutoff date for data collection, which was after the fiscal year was complete. Posttest scores were collected from 22 participants with no corresponding pretest. This was due to initiation of the program and completion of the pretest prior to the start of the data collection date range. Due to the inability to analyze the pre- and posttest scores of these participants’ data, these participants were eliminated from the study. Three participants were “reenrolled” in the program, meaning they began and completed services twice. One of these three participants began and completed both enrollments of services within the date range that data was collected; however, only the first set of pre- and posttest scores for this participant were used due to the need for a baseline data set. Because the second set of data for this participant were collected after the participant had previously fully completed the program, the second data score set was eliminated from analysis. Two of the three participants completed one enrollment of services during the date range of data collection and began the second enrollment during that time span, but the second enrollment of services ended after the end of the fiscal year. Therefore, for these participants, the pre- and posttest scores for first enrollment were included in the data set, but the second enrollment scores were eliminated because the scores included during second enrollment were pretest scores without corresponding posttest scores. This resulted in a total sample of 90 participants whose pre- and posttest scores were analyzed for the purposes of this research. Ethics All data were disclosed with no researcher access to any client data, demographic details, or identifying information. No client or participant data, confidentiality, or integrity was compromised throughout the conduct of this research. Measures The AAPI scale includes subscales which measure five family protective factor constructs: expectations of children, parental empathy towards children’s needs, use of corporal punishment, parent-child family roles, and children’s power and independence (Bavolek & Keene, 1999). Both the individual construct scores as well as the total cumulative inventory scores were analyzed for the study. The AAPI-2 has myriad potential uses, including testing treatment efficacy, assessing attitudes toward child rearing, designing a parenting treatment program or intervention to facilitate positive experiences between parents and adolescents, and to screen applicants for foster parenting as well as potential employees in childcare environments (Conners et al., 2006). One study found that the instrument is more accurate in identifying parents who were unlikely to abuse or neglect their children (Lawson et al., 2017). Although research assessing the psychometric properties of the AAPI-2 is limited, the extant literature has demonstrated average to good validity and reliability for this assessment tool (Conners et al., 2006; Lawson et al., 2017). Low standard errors of measure have also been demonstrated as well as both content- and construct-related validity and high internal reliability with an overall Chronbach alpha of 0.80 (Bavolek & Keene, 2005). Analytic Strategy The pre- and posttest scores of each protective factor for each family were analyzed utilizing a paired t-test utilizing SPSS version 26 (Ankarali et al., 2012). The differences in the pre- and posttest scores were analyzed for statistical significance and the effect size was calculated. Results
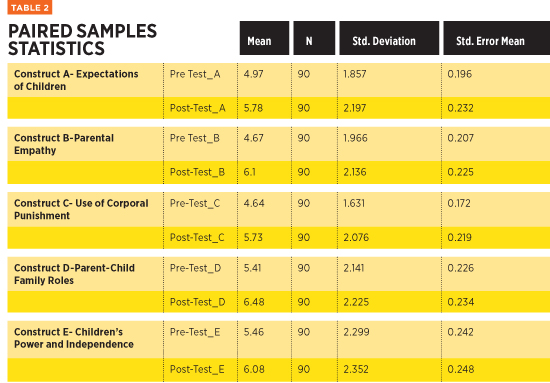
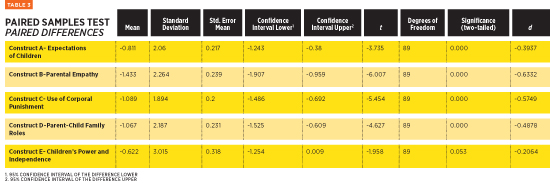
The largest change in pre- and posttest in this group of participants (n=90) was Construct B, parental empathy toward child’s needs. The smallest change in scoring—although still statistically significant (p=0.05)—was shown in Construct E, children’s power and independence. The effect sizes of each construct change were determined utilizing Cohen’s D (see Table 3). A two-tailed paired t-test demonstrates the largest significant changes in Construct B (M=-1.433, SD=2.264), t(89)=-6.007, p<0.001, d=-0.6332) as well as the smallest significant changes in Construct E (M=-0.622, SD=3.015), t(89)=-1.958, p=0.053, d=-0.2064).
Discussion and Implications for Practice The largest effect size noted in this sample was shown in Construct B, parental empathy toward child’s needs (d=0.63). Empathy is a foundational component of nurturing parenting; therefore, interventions that target all constructs involve empathy. For example, interventions geared toward appropriate discipline (use of corporal punishment, Construct C) incorporate empathy by means of engaging parents in reflecting on their own childhood experiences and disciplinary measures used by their own parents. The parents’ reflection process of their own lives and experiences of childhood utilizes an empathetic component as an avenue to cease corporal punishment and allow parents to move toward more appropriate disciplinary methods. Another example is a nurturing parenting lesson designed to target the development of appropriate expectations for children (Construct A). This lesson utilizes a reflection with the parents on their own experiences of realistic and unrealistic expectations by their own caregivers as children and how they have been positively and negatively affected in their past and present lives. Although this lesson plan was developed to address this construct, it uses empathy as a means to engage the parents, teach the lesson, and help the parents understand the material as well as conceptualize the competency. Many competencies are similar to these examples and include some empathetic component to teach the targeted construct, meaning this concept is reiterated throughout program delivery. The curriculum and constructs frequently relate to empathy and utilize this concept as a foundation on which to build on positive change. The frequency with which this concept is addressed throughout the interventions delivered during Nurturing Parenting explains the large effect size in this construct. The smallest effect size (d=0.21) within this sample was noted in Construct E (children’s power and independence). The implications for this outcome may relate to cultural issues and variance in interpretation of the questions posed by the AAPI among families. The demographic characteristics of families served at initial development of the Nurturing Parenting Program are very different from those of families currently receiving services. As needs change, agencies involved in service delivery are providing this intervention for families with a wide range of cultural backgrounds. However, extremely limited data exist on the adaptation of this home visiting intervention for cultural and demographical diversity. Therefore, language variation and translation may pose a skewed score result for culturally diverse families. This is particularly true for questions in the AAPI assessment and assignment of scores for Construct E. These questions tend to be culturally ambiguous and more subjective in nature. For example, one question assesses the parent’s viewpoint on the male child(ren) in the home becoming the “head of the household” in the absence of a father figure. This question is not only culturally subjective but also lacks consideration for same-sex female couples. Responses regarding traditional practices, rituals, and beliefs that are cultural in nature may be incorrectly screened as high-risk parenting. As a result, the lack of cultural adaptation may be a limitation for accurately assessing risk for child maltreatment. Language barriers and translation issues were also considerations in the efficacy of assessing child maltreatment risk in the context of Nurturing Parenting service delivery. Utilization of the AAPI presents subjectivity in responses of nonnative English-speaking families. Some Westernized “jargon,” colloquialisms, and euphemisms may pose challenges in translation. For example, one question in the scale assessing discipline poses the term “parents mean business,” which may be meaningless to members of some cultural groups. Some of the phrasing in the APPI may also leave room for subjectivity. For example, one question uses the term “strong-willed child,” which may be perceived as a positive or negative trait depending on the culture, roles, and experiences of the parents and family system. This also may be interpreted differently based on the gender of the child—it may be viewed more positively in a male than a female. When assessing families, the interpretation of these meanings and individual perceptions of words and phrases should be taken into consideration to ensure the most appropriate and beneficial foci of interventions during in-home sessions. To ensure understanding and mitigate the risk of misperception, staff involved in service delivery may consider engaging the family in clarification. After the assessment is complete, it is beneficial for staff to ask parents about the interpretation of questions, meaning making in their responses, and the family’s normative or cultural practices. This is of particular importance when serving culturally diverse families that may perceive concepts assessed by the tool as normative factors related to cultural identity. It is noteworthy that many questions throughout this tool use the word “children” with no age-related context. This has the potential to pose confusion in parents responding to the assessment questions. For example, the parent may be inclined to answer the question differently when pertaining to a 1-year-old than when referring to a 12-year-old. These discrepancies and subjectivity should be addressed by staff. Any confusion and interpretation issues should be noted to consider the implications for intervention options and provide optimal services that target and address the true areas of need for families served. To ensure consistency when clarifying and addressing interpretation and meaning making, staff should be involved in supervision. Supervision is a helpful tool in home visitation work, as the nature of the field may limit staff contact with coworkers or supervisors. Much of the time spent by home visiting workers is remote in the homes of clients and families, and supervisors or coworkers are not directly accessible during a session or immediately thereafter for processing. Previous research addressing this has found that supervision for staff in-home visitation fields is more effective if staff are observed either in person or by video recording of sessions (Cooley, 2011). Supervision has also been found to be more impactful for staff if the supervision content is more reflective rather than administrative (Casillas et al., 2016). Role playing and case staffing during supervision have been shown to contribute to implementation fidelity and service delivery consistency among staff as well as overall program effectiveness (Cooley, 2011). Interestingly, current program guidelines for nurturing parenting are absent of any standardization or recommendation for staff supervision practices. This may result in inconsistencies in service delivery and implementation methods. Supervisors should be trained to counsel staff with a consistent approach to ensure standardization in service delivery. This information should be considered in nurturing parenting supervision to address confusion or possible discrepancies among agencies that offer this program. Recommendations for Future Research Most of the research involving nurturing parenting program evaluation was conducted in the 1990s and early 2000s. It is noteworthy that the AAPI was originally developed and normed in 1979 and updated in 1999, which resulted in the AAPI-2 (Bavolek & Keene, 1999). Another update included additional demographic items, but no changes were made to the questions included in the assessment tool. As clients from wider demographics are served and the needs of families change, further research will need to evaluate what alterations should be implemented in nurturing parenting to accommodate more diverse child rearing issues that arise. To account for shifts in society and parenting needs, qualitative studies may be utilized for assessing the views and observations of parents who participate in this intervention and the perceptions in outcomes, benefits, and limitations. Currently, few qualitative studies of this program are present in the extant literature; this addition may provide new information and assist in the implementation of needed adaptations. It is worth mentioning that quantitative research on the Nurturing Parenting Program utilizes “sten scores” which are calculated through an algorithm created by the program developers. To avoid bias, an alternative method for interpreting assessment results may be considered for future research. Service delivery staff have also identified application discrepancies with this assessment tool. As needs and expectations for child rearing are shifting, modifications or updates of this tool may be necessary. Future research may consider evaluation through alternative assessment means, address the cultural application of this program, and examine subjective interpretation resulting in possibly inaccurate risk level identification for families involved in services. Further exploration in these areas may provide a more accurate identification of risk level and needs for families served to ensure the most effective and optimal interventions through nurturing parenting services. Limitations Formulation of research aims targeted more toward these factors may have yielded more applicable results with a more pervasive breadth and depth of findings. Furthermore, although nurturing parenting research is pervasive, most literature addresses the efficacy of the intervention exclusively. A gap exists in current literature addressing data collection, score interpretation, and cultural factors and therefore presents as a limitation in connecting the findings of this study to preexisting research. At the time of this study, the efficacy of nurturing parenting had been evaluated utilizing one method of scoring created by the developers of the intervention. This scoring method was also utilized in the current study, and future research may implement alternative scoring methods to evaluate efficacy to ensure consistency in current findings in the extant literature. Conclusion The initial purpose of this study was to evaluate the intervention and service delivery of one agency. Findings suggest that empathy is strongly impacted due to the recurrent incorporation of this concept throughout the material included in the nurturing parenting curriculum. Findings also reveal needs for future research in the data collection methods, assessment tool, and accommodation factors for diverse families. Gaps in research were also identified regarding cultural implications. As nurturing parenting continues to be implemented throughout various agencies across the nation, considerations should be made regarding appropriateness of curriculum, assessment, and service delivery in the context of changes and shifts in the needs of future children and families involved in the program. — Kalin Alvey, DSW, LCSW, CCTP, who received her Doctor of Clinical Social Work from the University of Tennessee, is certified in trauma treatment and veterinary social work, and holds a board-certified diplomate through the American Board of Clinical Social Work. She has clinical experience in child and family services, military and veteran populations, and an extensive history of trauma practice as well as active-duty military service as a behavioral health officer.
References Bailey, H. N., Moran, G., & Pederson, D. R. (2007). Understanding the transmission of attachment using variable- and relationship-centered approaches. Development & Psychopathology, 19(2), 313-343. Bavolek, S. J. (2006). The nurturing parenting programs. Park City, UT: Family Development Resources. Bavolek, S. J., & Keene, R. G. (2005). AAPI online development handbook: The Adult-Adolescent Parenting Inventory (AAPI-2) assessing high-risk parenting attitudes and behaviors. Park City, UT: Family Development Resource. Bavolek, S. J., & Keene, R. G. (1999). Adult-Adolescent Parenting Inventory: AAPI-2: assessing high-risk parenting attitudes and behaviors. Asheville, N.C.: Family Development Resources, Inc. Casillas, K. L., Fauchier, A., Derkash, B. T., & Garrido, E. F. (2016). Implementation of evidence-based home visiting programs aimed at reducing child maltreatment: A meta-analytic review. Child Abuse & Neglect, 53, 64-80. Conners, N. A., Whiteside-Mansell, L., Deere, D., Ledet, T., & Edwards, M. C. (2006). Measuring the potential for child maltreatment: The reliability and validity of the Adult Adolescent Parenting Inventory-2. Child Abuse & Neglect, 30(1), 39-53. Cooley, M. (2011). Short-term home visiting for parents. Journal of Family Social Work, 14(2), 179-188. Evans, R., Garner, P., & Honig, A. S. (2014). Prevention of violence, abuse and neglect in early childhood: a review of the literature on research, policy and practice. Early Child Development & Care, 184(9/10),1295-1335. Kim, H., Wildeman, C., Jonson-Reid, M., & Drake, B. (2017). Lifetime prevalence of investigating child maltreatment among US children. American Journal of Public Health, 107(2), 274-280. Lawson, M. A., Alameda-Lawson, T., & Byrnes, E. (2017). Analyzing the validity of the Adult-Adolescent Parenting Inventory for low-income populations. Research on Social Work Practice, 27(4), 441-455. Lo, C. K. M., Ko L. C., & Ip, P. (2019). Insecure adult attachment and child maltreatment: A meta-analysis. Trauma, Violence & Abuse, 20(5), 706-719. Madigan, S., Moran, G., Schuengel, C., Pederson, D. R., & Otten, R. (2007). Unresolved maternal attachment representations, disrupted maternal behavior and disorganized attachment in infancy: Links to toddler behavior problems. Journal of Child Psychology & Psychiatry, 48(10), 1042-1050. Olds, D. L., Robinson, J., Pettitt, L., Luckey, D. W., Holmberg, J., Ng, R. K., & Henderson, C. R., Jr. (2004). Effects of home visits by paraprofessionals and by nurses: Age 4 follow-up results of a randomized trial. Pediatrics, 114(6), 1560-1568. Peterson, C., Florence, C., & Klevens, J. (2018). The economic burden of child maltreatment in the United States, 2015. Child Abuse & Neglect, 86, 178-183. Stovall-McClough, K. C., & Cloitre, M. (2006). Unresolved attachment, PTSD, and dissociation in women with childhood abuse histories. Journal of Consulting & Clinical Psychology, 74(2), 219-228. |
 Child Maltreatment Services
Child Maltreatment Services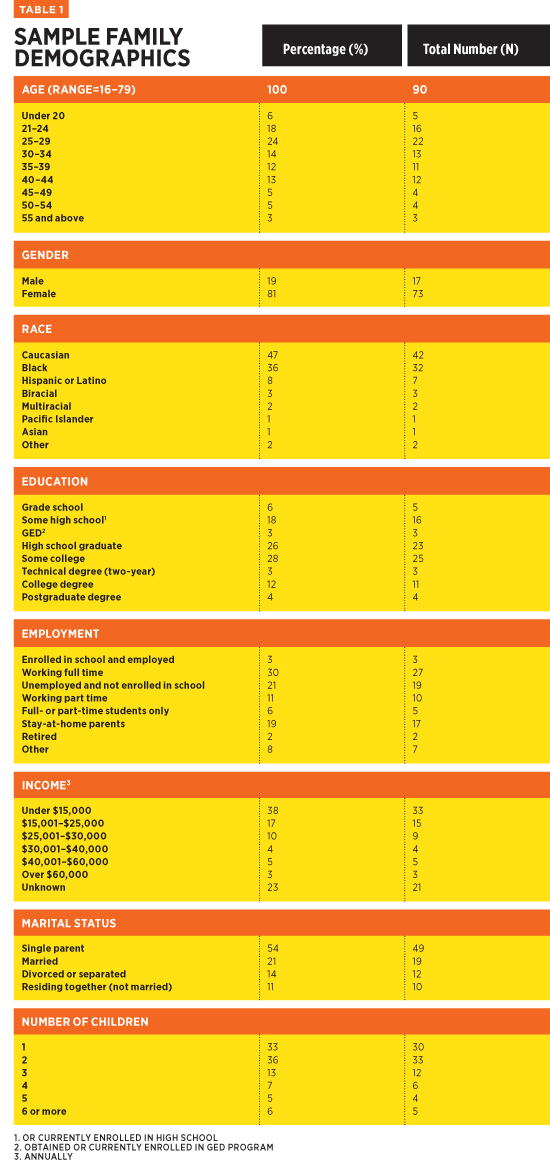

Great Valley Publishing Company
1721 Valley Forge Road #486
Valley Forge, PA 19481
1721 Valley Forge Road #486
Valley Forge, PA 19481